

Vaccines for Children (5-11 years old)
Vaccines for Children (5-11 years old)
The VRBPAC meeting that approved vaccines for young kids did not at all sound like people who are mindlessly pro-vaccine

Two weeks ago, the FDA hosted the Vaccines and Related Biological Products Advisory Committee meeting to review the evidence submitted by Pfizer in support of making their COVID vaccine (which they call Comirnaty but I refuse to use that name because it is hard to say and eye-rollingly goofy) available to children aged 5-11.
The result of this meeting was 14 votes in favor of making the vaccine available, one abstention, and zero votes against it. You can watch the entire excruciatingly long discussion on YouTube. You can also peruse my very spotty notes that I took and reviewed as I was writing this.
I wanted to write about these meetings because we often only see the end result (the vote) that comes from these meetings but that ends up missing a lot of the important information. It also makes people angry or happy that their vision of the world was rebuked or reinforced. If you think that, as a general rule, kids probably don’t need to get the COVID vaccine, then looking at a 14-0-1 feels like you were told that you were wrong. If, instead, you think the FDA should have approved this already and we need to get the COVID vaccine on the school vaccine schedules already, then you will feel like this result reinforces your position.
Watching this discussion from beginning to end is an important task for me because it helps me connect with the FDA process in a more intimate way. I can see the doctors discussing, debating, questioning, and reconsidering. I think that, were I a voting member, I probably would have voted “yes” for the exact same reason these doctors voted “yes”.
The Big Question
Let’s start at the end: The question on which the committee members voted was:
The moderator made it clear that this was the specific question they were voting on and that their vote had to be in answer to this question. This actually riled the committee members somewhat (though in a fairly lighthearted way). Dr Michael Kurilla mentioned that he resented the binary presentation of the question when the question of the application of the vaccine to children ages 5-11 was much more complex than “do the benefits outweigh the risks”. Dr Michael Nelson mentioned that he understood why the question was asked this way, but he didn’t like it and that every yes vote would probably come with a caveat.
To best understand why this question has caused so much consternation, we have to understand what the risks and benefits are.
The Case For The COVID Vaccine For Kids
The case for giving this vaccine to healthy kids is a much tougher case than it was for adults. The first difficulty is that the adult trial was a massive 36,000 person study that found that the vaccine was effective at reducing rates of symptomatic COVID as well as the severity of the disease.
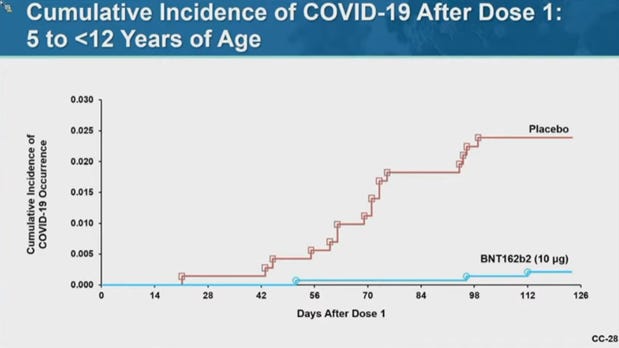
The similar trials for children involved a much smaller trial size of 2,268 participants. They trial reduced the vaccine dosage by two thirds (from 30 micrograms to 10 for young children). During the duration of the trial, they found the vaccine was about as effective in case reduction for children as it had been for adults.
The big difference between kids and adults is that severe COVID in children is far less common than in adults. The “gold standard” for the vaccine application in adults has always been “does this prevent severe disease?” We had enough data in the adult trial to answer this question but we don’t know if this is true for children.
Now I’m going to criticize on my own statement there: We don’t *know* if it is true because, during the study, there were no severe cases among any of the study participants. There were no severe cases in the placebo group or in the vaccinated group. This doesn’t mean that the vaccine *doesn’t* reduce disease severity. We certainly expect that it would reduce rates of severe disease in kids, but we don’t have the data to tell us how much.
Judged against this benefit is the now-known risk of myocarditis among younger people. There was a really fantastic presentation at 1:28 from Dr Matthew Oster on myocarditis in which he goes through a lot of data on how frequent myocarditis is from vaccine administration, from COVID cases, and from background incidence.
The very story short is that background myocarditis is most common among teenage boys and that the risk from the vaccine seems to be highest in that age group (16-18 year old boys). It is less common among children in the 5-11 age group and we don’t yet have data on how much the vaccine might increase that risk. Just as there were no COVID hospitalizations in this study due to how rare complications in this age range, there were also no myocarditis cases reported among the participants for vaccine trial due to the rarity of this adverse event. But, based on what we know about myocarditis and the vaccine, we should expect there would be *some* increase in cases.
The Case Of The Confusing Model
It was in trying to model possible scenarios to judge the risk against the reward that the waters started to get muddy. This slide in particular caused a lot of concern because it showed that vaccine-induced myocarditis ICU stays could be high enough in this age group that it rivals the COVID ICU stays that the vaccine prevent.
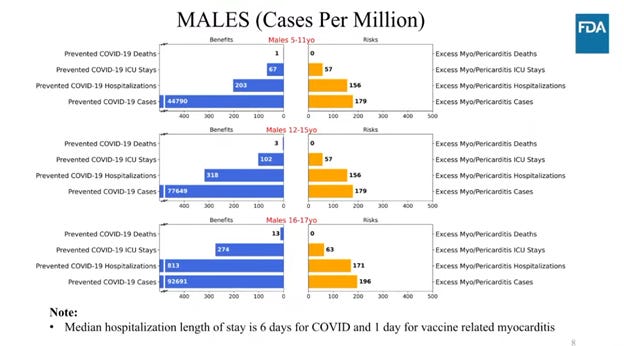
I’ve seen this chart a lot on twitter. There are a lot of problems with this chart. The first is that this chart alone is way out of context. This is one chart in a series of charts that looked like this that were intended to balance a number of different scenarios. They looked at scenarios for high COVID incidence, higher-than-expected vaccine efficacy, and lower myocarditis rates.
This particular scenario (Scenario 3) assumed particularly low COVID cases (similar to what we were seeing last June) and simply took the myocarditis risk that we have measured for 12-15 year old boys and applied to directly to 5-11 year old boys. The modelers did this as an intentional over-estimate to try to inflate the estimate of risk in order to demonstrate that they thought that even in the best case COVID scenario and the worst case myocarditis scenario, the risk-reward balance was about even.
But the model itself was so simplistic that it drew some critical questions from the committee members.
Did the model account for the immunity of kids who already caught COVID? No.
Did they account for the fact that 20% of pediatric COVID hospitalizations were not due to COVID but incidental infections? No.
Have we done modeling like this for any other vaccine so we can compare this vaccine’s risk-reward to other existing vaccines? No.
Does this model account for waning immunity? No.
Does this model account for additional risk if children need booster shots? No.
The model is a simple calculation of known COVID rates multiplied against the reported efficacy of the vaccine and then compared to the known myocarditis risk from an older age group. This means that some of the scenarios (specifically Scenario 3 above) are probably overly pessimistic and the most stark scenario (Scenario 2) is probably overly optimistic. But I got the sense throughout the meeting that the committee members were really digging into the evidence and asking hard questions. There was a very sharp sense of skepticism and a deep concern that all the data be considered and the best decisions be made.
The Final Determination
The very best parts of the discussion came toward the end (after about 6:50:00 in the video) as the committee debated the need for the vaccine. Several committee members noted that making the vaccine available for high risk kids is a good idea. Children with existing lung conditions or who suffer from comorbities like obesity or immunosuppression could benefit enormously from having some effective level of protection from COVID. These kids make up a large percentage of the COVID deaths in this age group. Giving them an option for protection is a big deal.
At the same time, several doctors specifically stated that they thought vaccine mandates for this age group would not be appropriate. Dr Cody Meissner expressed concern states and school districts would misinterpret their vote as an invitation to mandate the vaccine for school children. He opposed that idea and made a specific note that this vaccine was not at all like the MMR vaccine that is required at schools. Dr James Hildreth went so far as to say that the most appropriate path forward for many children would be to do nothing at all even after the vaccine is available.
There seemed to be a resilient faith among the doctors in this discussion that the only appropriate way to move forward would be to make the vaccine available and then trust parents and caregivers to take into consideration all the risks and make the right decisions given the evidence that is available.
Hearing them say this is so strange to me because that is exactly my position. I often allow myself to get carried away with the online rhetoric but I think the clearest response to this is to trust people to do what is right for themselves and their loved ones.
Does your child have a chronic condition that makes COVID a particularly dangerous disease? You should have access to a vaccine to keep her safe.
Is your child recently recovered from COVID and otherwise healthy? It is the opinion of the experts from the FDA that vaccinating them confers so little benefit that is outweighed by even the small known risks.
Mandates ignore this consideration. The best path forward is to let people make their own decisions and assess their own risks.
Borrowing Trouble
Perhaps I’m borrowing trouble with this thought, but it worries me that the sense of what is happening online and in the news is a huge disconnect from what I hear when I dip my head into these expert reviews. I love these conversations. I love listening to them, hearing from these experts debate and fight with how to help the public make the best decisions.
There is a sense among many cautious parents that a vote to approve the vaccine for 5-11 year olds is the same as endorsing a COVID vaccine mandate for school attendance. This is not an ill-founded fear; California seems likely to demand COVID vaccinations for all school children in the next school year.
It’s important to highlight that a COVID vaccine mandate for children is not “listening to the science”. It is ignoring the scientists and doctors and disregarding their warnings and concerns in search of an easy answer. They are as worried as parents are about the misapplication of this approval. But they have to balance that against the benefits this vaccine can provide to vulnerable children. They’re frustrated by this and they think parents should be given enormous latitude in making the best decisions for their kids.
But they are also gatekeepers and they can’t open the gate just a little bit. The ACIP tried that with their limited booster recommendation and their advice was disregarded by the Biden administration. They are in a difficult spot and I can sense their frustration throughout this meeting. I wish this information was more widely known because I think that, if people knew the details of how the FDA VRBPAC came to this decision, they would feel like they were being heard and have more confidence in the process (which we desperately need right now).
I find encouragement in the recommendations from the committee. If you’re anxious about vaccinating your healthy child, you’re listening to the science. If you think that the natural immunity your kid got 2 months ago is good enough, you’re listening to the science. If you want to get a vaccine for your kid b/c you think the risks are small enough to tolerate, you’re listening to the science. For kids, there is an incredibly wide range of reasonable approaches and no one should be shamed or judged for the decision they make for their family.
That is what the scientists said. I’m just the messenger.
Alice’s Wonderland
This is the first “Alice” cartoons that Walt Disney created. In order to combine live-action with animation, he created a matting technology that was able to combine film exposures in such a way that you could have live-action in a portion of the screen and animated action in another portion. That is how he got Alice to inhabit an animated world, by giving her a portion of the screen to act in while the animation took up the rest of the frame.
This short starts with young Alice invading the animators room to watch them draw their cartoons. After some silly demonstrations of what cartoons can do, we’re transported to Alice’s dream where she must entertain mouse mayors, participate in grand parades, and fight off animated lions.
Part of the joy of this cartoon is wondering how they did it. Yes, Disney’s matting technology was impressive, but there are a few scenes where he really pushed that strategy to the limit. This was indicative of Disney’s innovative spirit. When this cartoon was made, Walt Disney was 23 years old and completely unsatisfied with simply making a good cartoon with astounding technology. Even then, he had to push the tech to its limit and challenge his animators to do their best.
As always, you have written a thoughtful essay. However I would like to quibble with one of your points, specifically that the gold standard of the vaccines was always to prevent severe disease . It was not presented that way as I recall; I believe it was presented as a way to end the pandemic and as highly preventive of infection, hospitalization and death. With the passage of time it has become clear it does not prevent infection. Studies that want to continue to claim that it reduces hospitalization and death due to Covid need to adjust for multiple confounders, including but not limited to: age, gender, ethnicity of the patient; Comorbid illnesses known to affect survival; vaccination status that includes which vaccine and the date of the vaccination as we know that effectiveness of the vaccines declines overtime. I would also like to know what early treatments, if any, the Covid patients received. This is a rather tall order. In the meantime, I am hoping we get additional vaccines to choose from, and in particular ones that directly target the Delta variant.
You can't listen to science because science cannot speak. It's not an entity, it's a process for learning about the world.
Sounds to me like they knew that this would result in way too many kids being given these things when they shouldn't and they did it anyway. That to me is irresponsible.